Disclaimer: This article is purely for education purpose & consent has been taken from the patients to display the images/ video. Some of the pictures & diagrams are uploaded from google images. Would like to thank all patients, contributors & owners for the google images for their pictures/video to be used in this article.
Haematocolpos
What is Haematocolpos: It is a medical condition in which the vagina (colpos) is filled/pooled with menstrual blood. It is due to the blockage of menstrual blood flow. The word hematocolpos stands for 'an accumulation of blood within the vagina'. It is often caused by obstruction to the outflow of menstrual blood flow through the vagina. Haematometra which is the collection of blood in the uterus is sometime related with haematocolpos. The intense pressure & back flow of the obstructed blood leads to formation of Haematometra. In this articles, i will confine our discussion to simple Haematocolpos only. Below are example causes of haematocolpos.

a. Imperforate hymen


b. vaginal atresia






c. transverse septum


d. Mullerian Duct Anomalies


Typical Clinical presentation are as below: all these case were manged by me. These cases presented in different scenarios with different physical findings. Tha manage are tailored based on the underlying cause/pathology and was dealt accordingly.
Case 1:
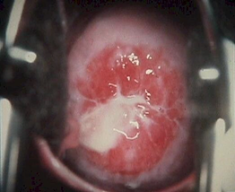
A 12 year old girl, presented to casualty with severe lower abdominal pain. She has this cyclical pain for few months before. She has not attain menarche yet. On examination, the secondary sex characteristics are present. On abdominal examination, there was a 16 week size pelvic mass & its tender on palpation. Perineal examination, there was bluish bulging from the vaginal out let. Pelvic Ultrasound sound showed a large Haematocolpos. The uterus was normal with slight thickened ET & there was some fluid in POD. DX: Imperforate Hymen. Investigation is usually pelvic ultrasound is sufficient. Treatment is usually a simple cruciate incision or elliptical incision of the hymen. Hymen can usually be spaced (hymen spacing surgery). In this case a cruciate incision was made. The staled blood was drained passively. Patient recovered uneventfully.


Case 2:
13 year old girl presented to the casualty with primary amenorrhea & cyclical abdominal pain and difficulty pass urine. On examination, the sexual characteris was normal. The abdomen was distended. Vaginal examination. there were no vaginal opening. There was no perineal bulging. PR there was a gap in between the forchette and the the upper border of the vaginal. The pelvic ultrasound showed a large haematocolpos and some haematometra ( blood collection in the uterus). DX: Vaginal Atresia







Treatment: EUA, Excision of the septum & Diagnostic Laparoscopy was carried out

For the women who have an imperforate hymen, a minor surgery is sufficient. An incising for the hymenic membrane or hymenotomy is sufficient to facilitate menstrual flow. In some case with tight outlet, patients may be required to insert dilators into the vagina for a few minutes each day for a few days post the surgery to avoid the incision being closed on its own or to maintain it patency. The surgical correction of a transverse septum and vaginal atresia can be difficult if the surgery is not carefully planned. Postoperative complications, such as vaginal stenosis and re-obstruction can occur, especially when the septum/vagina is thick. In such cases long term dilation with vaginal dilators may be necessary.The thickness and location of the septum is most commonly evaluated by transperineal ultrasound or MRI before attempting its resection. Mullerian duct anomalies can be changing & the surgical treatment planned need to be tailored toward relieve the acute symptoms & long term maintenance for the sexual & reproduction function in such patients. In such cases a preoperative assessment with imaging techniques and multi discipline approach may be necessary to provide effective & long term good outcome.